

Writing Nursing Care Plan (NCP) Essays
Writing the best nursing care plan requires a step-by-step approach to correctly complete the parts needed for a care plan. In this tutorial, we have the ultimate database and list of nursing care plans (NCP) and NANDA nursing diagnosis samples for our student nurses and professional nurses to use — all for free! Components, examples, objectives, and purposes of a care plan are included together with an elaborate guide on how to write an awesome nursing care plan or a template for your unit.
- What is a nursing care plan?
- Types of Nursing Care Plans
- Objectives
- Purposes of a Nursing Care Plan
- Components
- Care Plan Formats
- Student Care Plans
- Writing a Nursing Care Plan
- Step 1: Data Collection or Assessment
- Step 2: Data Analysis and Organization
- Step 3: Formulating Your Nursing Diagnoses
- Step 4: Setting Priorities
- Step 5: Establishing Client Goals and Desired Outcomes
- Short Term and Long Term Goals
- Components of Goals and Desired Outcomes
- Step 6: Selecting Nursing Interventions
- Types of Nursing Interventions
- Step 7: Providing Rationale
- Step 8: Evaluation
- Step 9: Putting it on Paper
- Nursing Care Plan List
- Basic Nursing and General Care Plans
- Surgery and Perioperative Care Plans
- Maternal and Newborn Care Plans
- Pediatric Nursing Care Plans
- Cardiac Care Plans
- Endocrine and Metabolic Care Plans
- Gastrointestinal
- Genitourinary
- Hematologic and Lymphatic
- Infectious Diseases
- Integumentary
- Mental Health and Psychiatric
- Neurological
- Musculoskeletal
- Ophthalmic
- Respiratory
- References and Sources
What is a nursing care plan?
A nursing care plan (NCP) is a formal process that includes correctly identifying existing needs, as well as recognizing potential needs or risks. Care plans also provide a means of communication among nurses, their patients, and other healthcare providers to achieve health care outcomes. Without the nursing care planning process, quality and consistency in patient care would be lost.

Nursing care planning begins when the client is admitted to the agency and is continuously updated throughout in response to client’s changes in condition and evaluation of goal achievement. Planning and delivering individualized or patient-centered care is the basis for excellence in nursing practice.
Types of Nursing Care Plans
Care plans can be informal or formal: Informal nursing care plan is a strategy of action that exists in the nurse‘s mind. A formal nursing care plan is a written or computerized guide that organizes information about the client’s care. Formal care plans are further subdivided into standardized care plan, and individualized care plan: Standardized care plans specify the nursing care for groups of clients with everyday needs. Individualized care plans are tailored to meet the unique needs of a specific client or needs that are not addressed by the standardized care plan.
Objectives
The following are the goals and objectives of writing a nursing care plan:
- Promote evidence-based nursing care and to render pleasant and familiar conditions in hospitals or health centers.
- Support holistic care which involves the whole person including physical, psychological, social and spiritual in relation to management and prevention of the disease.
- Establish programs such as care pathways and care bundles. Care pathways involve a team effort in order to come to a consensus with regards to standards of care and expected outcomes while care bundles are related to best practice with regards to care given for a specific disease.
- Identify and distinguish goals and expected outcome.
- Review communication and documentation of the care plan.
- Measure nursing care.
Purposes of a Nursing Care Plan
The following are the purposes and importance of writing a nursing care plan:
- Defines nurse’s role. It helps to identify the unique role of nurses in attending the overall health and well-being of clients without having to rely entirely on a physician’s orders or interventions.
- Provides direction for individualized care of the client. It allows the nurse to think critically about each client and to develop interventions that are directly tailored to the individual.
- Continuity of care. Nurses from different shifts or different floors can use the data to render the same quality and type of interventions to care for clients, therefore allowing clients to receive the most benefit from treatment.
- Documentation. It should accurately outline which observations to make, what nursing actions to carry out, and what instructions the client or family members require. If nursing care is not documented correctly in the care plan, there is no evidence the care was provided.
- Serves as guide for assigning a specific staff to a specific client. There are instances when client’s care needs to be assigned to a staff with particular and precise skills.
- Serves as guide for reimbursement. The medical record is used by the insurance companies to determine what they will pay in relation to the hospital care received by the client.
- Defines client’s goals. It does not only benefit nurses but also the clients by involving them in their own treatment and care.
Components
A nursing care plan (NCP) usually includes nursing diagnoses, client problems, expected outcomes, and nursing interventions and rationales. These components are elaborated below:
- Client health assessment, medical results, and diagnostic reports. This is the first measure in order to be able to design a care plan. In particular, client assessment is related to the following areas and abilities: physical, emotional, sexual, psychosocial, cultural, spiritual/transpersonal, cognitive, functional, age-related, economic and environmental. Information in this area can be subjective and objective.
- Expected client outcomes are outlined. These may be long and short term.
- Nursing interventions are documented in the care plan.
- Rationale for interventions in order to be evidence-based care.
- Evaluation. This documents the outcome of nursing interventions.
Care Plan Formats
Nursing care plan formats are usually categorized or organized into four columns: (1) nursing diagnoses, (2) desired outcomes and goals, (3) nursing interventions, and (4) evaluation. Some agencies use a three-column plan wherein goals and evaluation are in the same column. Other agencies have a five-column plan that includes a column for assessment cues.
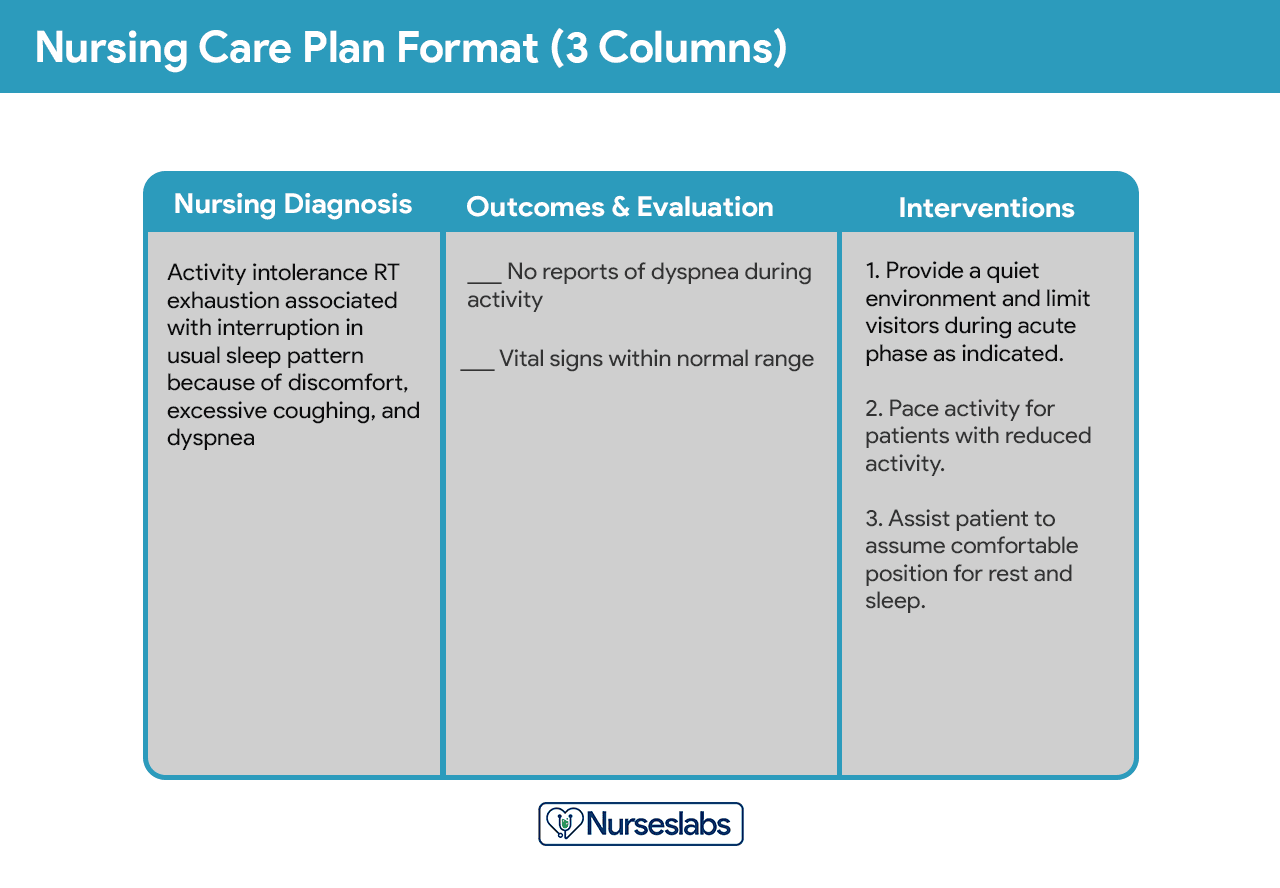
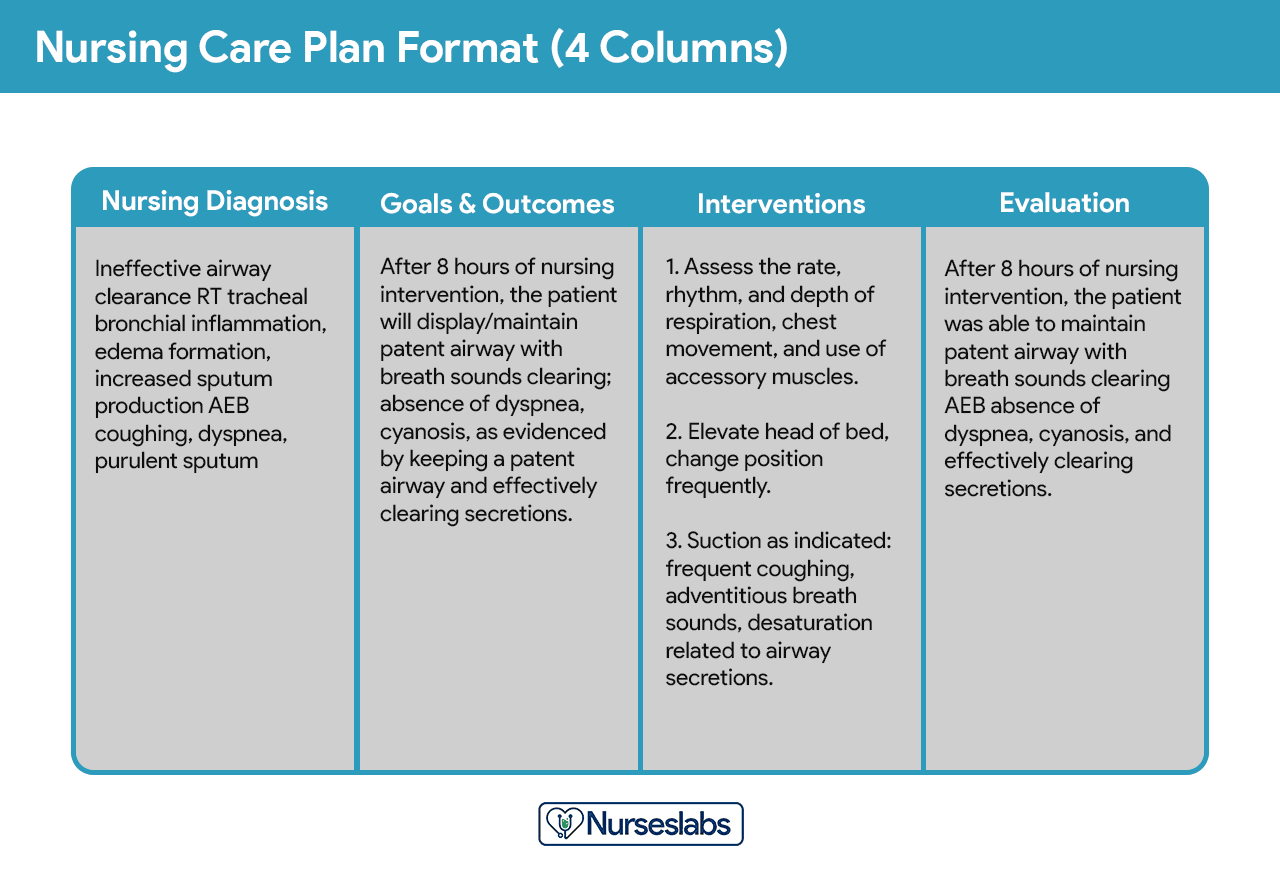
Below is a document containing sample templates for the different nursing care plan formats. Please feel free to edit, modify, and share the template.
Download Nursing Care Plan Templates and Formats
Student Care Plans
Student care plans are more lengthy and detailed than care plans used by working nurses because they are a learning activity for the students.

Care plans by student nurses are usually required to be handwritten and have an additional column for “Rationale” or “Scientific Explanation” after the nursing interventions column. Rationales are scientific principles that explains the reasons for selecting a particular nursing interventions.
Writing a Nursing Care Plan
How do you write a nursing care plan (NCP)? Just follow the steps below to develop a care plan for your client.
Step 1: Data Collection or Assessment
The first step in writing a nursing care plan is to create a client database using assessment techniques and data collection methods (physical assessment, health history, interview, medical records review, diagnostic studies). A client database includes all the health information gathered. In this step, the nurse can identify the related or risk factors and defining characteristics that can be used to formulate a nursing diagnosis. Some agencies or nursing schools have their own assessment formats you can use.ADVERTISEMENTS
Step 2: Data Analysis and Organization
Now that you have information about the client’s health, analyze, cluster, and organize the data to formulate your nursing diagnosis, priorities, and desired outcomes.
Step 3: Formulating Your Nursing Diagnoses
NANDA nursing diagnoses are a uniform way of identifying, focusing on, and dealing with specific client needs and responses to actual and high-risk problems. Actual or potential health problems that can be prevented or resolved by independent nursing intervention are termed nursing diagnoses. We’ve detailed the steps on how to formulate your nursing diagnoses in this guide: Nursing Diagnosis (NDx): Complete Guide and List for 2019
Step 4: Setting Priorities
Setting priorities is the process of establishing a preferential sequence for address nursing diagnoses and interventions. In this step, the nurse and the client begin planning which nursing diagnosis requires attention first. Diagnoses can be ranked and grouped as to having a high, medium, or low priority. Life-threatening problems should be given high priority.

Client’s health values and beliefs, client’s own priorities, resources available, and urgency are some of the factors the nurse must consider when assigning priorities. Involve the client in the process to enhance cooperation.
Step 5: Establishing Client Goals and Desired Outcomes
After assigning priorities for your nursing diagnosis, the nurse and the client set goals for each determined priority. Goals or desired outcomes describe what the nurse hopes to achieve by implementing the nursing interventions and are derived from the client’s nursing diagnoses. Goals provide direction for planning interventions, serve as criteria for evaluating client progress, enable the client and nurse to determine which problems have been resolved, and help motivate the client and nurse by providing a sense of achievement.

One overall goal is determined for each nursing diagnosis. The terms goal, outcome, and expected outcome are oftentimes used interchangeably.
Short Term and Long Term Goals
Goals and expected outcomes must be measurable and client-centered. Goals are constructed by focusing on problem prevention, resolution, and/or rehabilitation. Goals can be short term or long term. In an acute care setting, most goals are short-term since much of the nurse’s time is spent on the client’s immediate needs. Long-term goals are often used for clients who have chronic health problems or who live at home, in nursing homes, or extended care facilities.
- Short-term goal – a statement distinguishing a shift in behavior that can be completed immediately, usually within a few hours or days.
- Long-term goal – indicates an objective to be completed over a longer period, usually over weeks or months.
- Discharge planning – involves naming long-term goals, therefore promoting continued restorative care and problem resolution through home health, physical therapy, or various other referral sources.
Components of Goals and Desired Outcomes
Goals or desired outcome statements usually have the four components: a subject, a verb, conditions or modifiers, and criterion of desired performance.
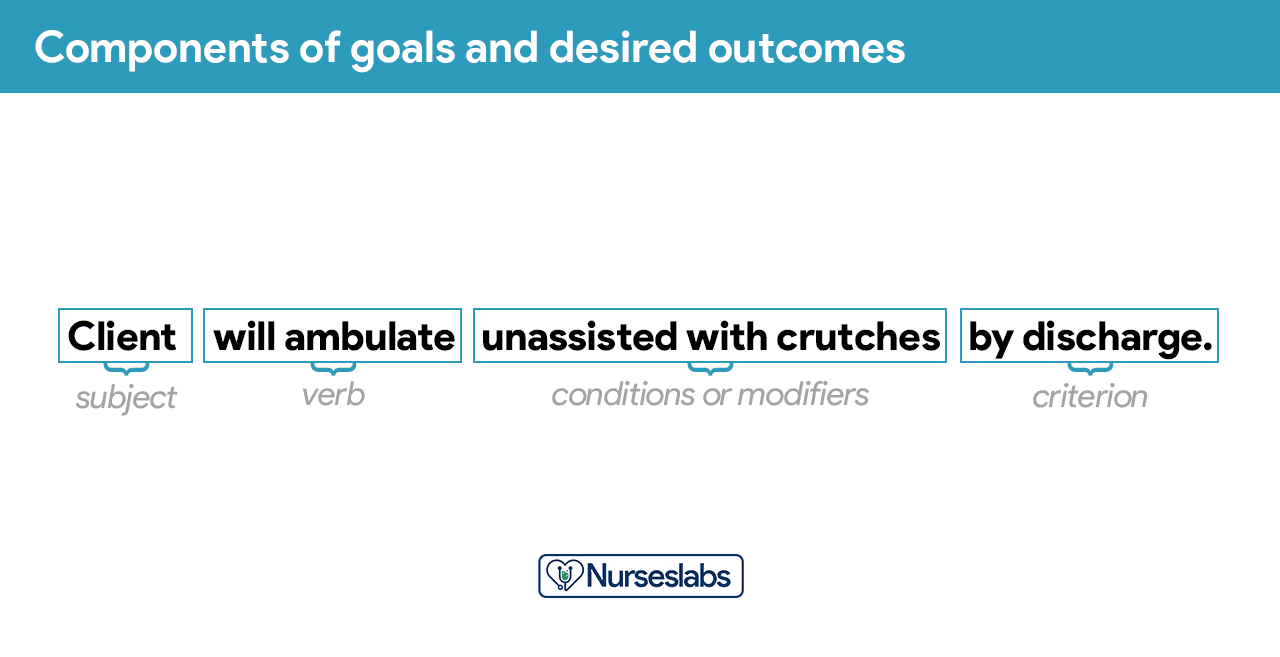
- Subject. The subject is the client, any part of the client, or some attribute of the client (i.e., pulse, temperature, urinary output). That subject is often omitted in writing goals because it is assumed that the subject is the client unless indicated otherwise (family, significant other).
- Verb. The verb specifies an action the client is to perform, for example, what the client is to do, learn, or experience.
- Conditions or modifiers. These are the “what, when, where, or how” that are added to the verb to explain the circumstances under which the behavior is to be performed.
- Criterion of desired performance. The criterion indicates the standard by which a performance is evaluated or the level at which the client will perform the specified behavior. These are optional.
When writing goals and desired outcomes, the nurse should follow these tips:
- Write goals and outcomes in terms of client responses and not as activities of the nurse. Begin each goal with “Client will […]” help focus the goal on client behavior and responses.
- Avoid writing goals on what the nurse hopes to accomplish, and focus on what the client will do.
- Use observable, measurable terms for outcomes. Avoid using vague words that require interpretation or judgment of the observer.
- Desired outcomes should be realistic for the client’s resources, capabilities, limitations, and on the designated time span of care.
- Ensure that goals are compatible with the therapies of other professionals.
- Ensure that each goal is derived from only one nursing diagnosis. Keeping it this way facilitates evaluation of care by ensuring that planned nursing interventions are clearly related to the diagnosis set.
- Lastly, make sure that the client considers the goals important and values them to ensure cooperation.
Step 6: Selecting Nursing Interventions
Nursing interventions are activities or actions that a nurse performs to achieve client goals. Interventions chosen should focus on eliminating or reducing the etiology of the nursing diagnosis. As for risk nursing diagnoses, interventions should focus on reducing the client’s risk factors. In this step, nursing interventions are identified and written during the planning step of the nursing process; however, they are actually performed during the implementation step.
Types of Nursing Interventions
Nursing interventions can be independent, dependent, or collaborative:
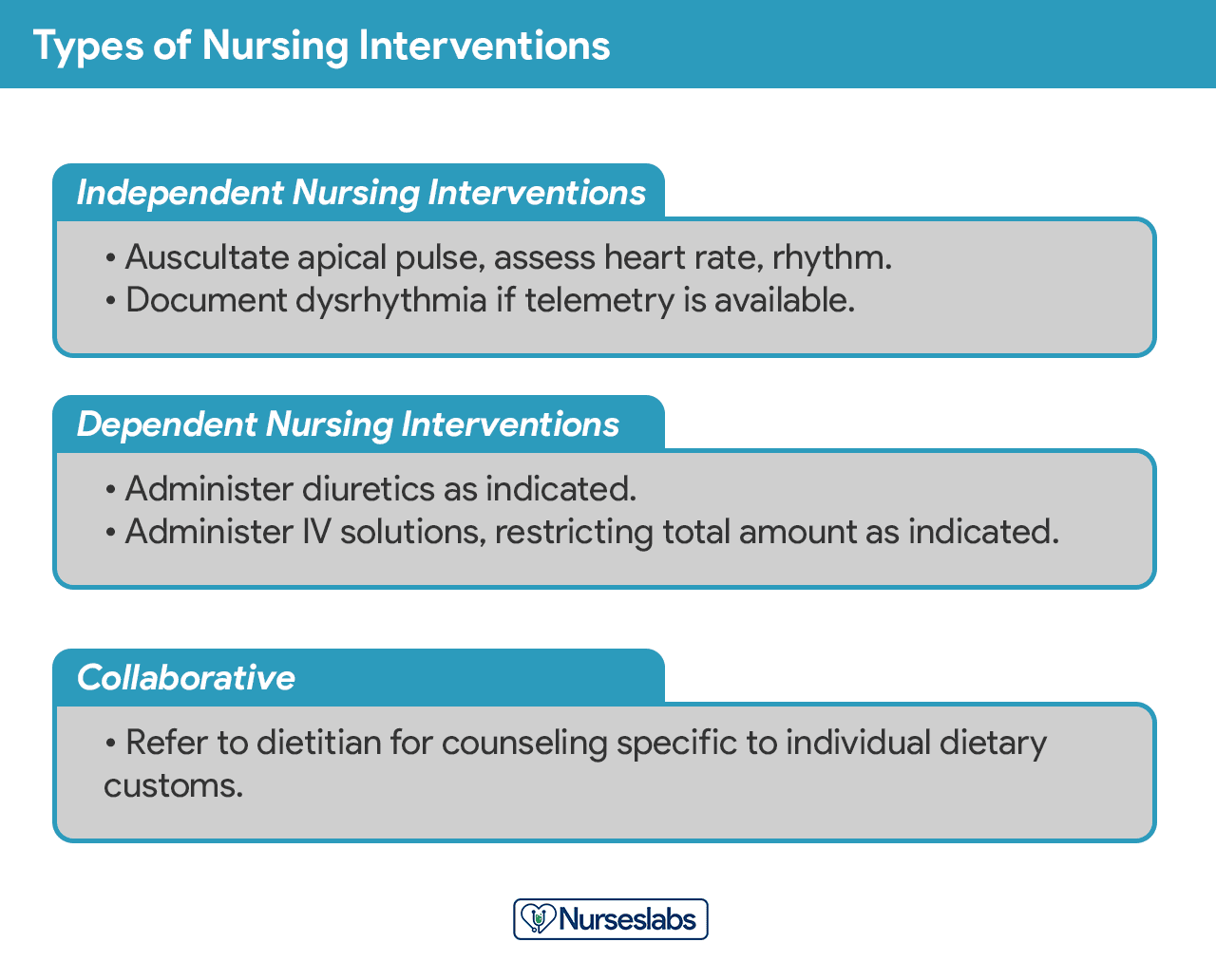
- Independent nursing interventions are activities that nurses are licensed to initiate based on their sound judgement and skills. Includes: ongoing assessment, emotional support, providing comfort, teaching, physical care, and making referrals to other health care professionals.
- Dependent nursing interventions are activities carried out under the physician’s orders or supervision. Includes orders to direct the nurse to provide medications, intravenous therapy, diagnostic tests, treatments, diet, and activity or rest. Assessment and providing explanation while administering medical orders are also part of the dependent nursing interventions.
- Collaborative interventions are actions that the nurse carries out in collaboration with other health team members, such as physicians, social workers, dietitians, and therapists. These actions are developed in consultation with other health care professionals to gain their professional viewpoint.
Nursing interventions should be:ADVERTISEMENTS
- Safe and appropriate for the client’s age, health, and condition.
- Achievable with the resources and time available.
- Inline with the client’s values, culture, and beliefs.
- Inline with other therapies.
- Based on nursing knowledge and experience or knowledge from relevant sciences.
When writing nursing interventions, follow these tips:
- Write the date and sign the plan. The date the plan is written is essential for evaluation, review, and future planning. The nurse’s signature demonstrates accountability.
- Nursing interventions should be specific and clearly stated, beginning with an action verb indicating what the nurse is expected to do. Action verb starts the intervention and must be precise. Qualifiers of how, when, where, time, frequency, and amount provide the content of the planned activity. For example: “Educate parents on how to take temperature and notify of any changes,” or “Assess urine for color, amount, odor, and turbidity.”
- Use only abbreviations accepted by the institution.
Step 7: Providing Rationale
Rationales, also known as scientific explanation, are the underlying reasons for which the nursing intervention was chosen for the NCP.
Writing Nursing Care Plan

- Confidentiality & Authenticity Guaranteed
- Plagiarism Free Content Guarantee
- APPROVEDSCHOLARS Guarantee Timely Delivery of All Papers
- Quality & Reliability
- Papers Written from Scratch and to Your Instructions
- Qualified Writers Only
- APPROVEDSCHOLARS Allow Direct Contact With Your Writer
- Using APPROVEDSCHOLARS.COM Means Keeping Your Personal Information Secure
- 24/7 Customer Support
WHY APPROVEDSCHOLARS.COM
GET QUALITY ESSAY HELP AT: https://www.approvedscholars.com/
ORDER A PAPER WRITTEN FROM SCRATCH AND TO YOUR EXACT INSTRUCTIONS (APPROVEDSCHOLARS.COM – For 100% Original Content)
